




Anatomical and functional changes in the upper urinary tract in patients with muscle invasive bladder cancer
Summary. The paper presents the results of analysis of a comprehensive radiation examination of 250 patients with muscle invasive bladder cancerthat, in 75 cases, was complicated by ureterohydronephrosis. The possibilities of MR urography were studied with the use of paramagnetic contrast agents and forced diuresis in the diagnosis of anatomical and functional changes in the upper urinary tract.
Introduction
 It is known that in the diagnosis of diseases of upper urinary tract radiation methods play a significant role in influencing the formation of diagnosis and subsequent treatment strategy [1].
It is known that in the diagnosis of diseases of upper urinary tract radiation methods play a significant role in influencing the formation of diagnosis and subsequent treatment strategy [1].
The discovery in 1929 of excretory urography by Binz and Rath was an outstanding achievement in science that influenced the development of urology and nephrology, and is now widely used in various algorithms in the examination of patients and in different modifications [2]. However, there is a rather large group of patients in whom the excretory urography is little informative or its application is impossible, namely, with a blocked kidney, renal insufficiency, and renal colic. There are also well-known contraindications to the use of iodine-containing contrast agents: hyperthyrosis, expressed hepatic and renal failure, hypertension in decompensation stage, pregnancy, allergy to iodine. In addition, traditional radiographic methods give an idea of the anatomical and functional status of the upper urinary tract, but the possibility of identifying the causes of urinary tract obstruction, tumors of the ureters and of the urinary tract, is limited. Besides, it is necessary to consider radiation exposure on the patient. It should be noted that for a long time it was impossible to get an image of upper urinary tract without using ionizing radiation and iodine-containing contrast media infusion. But at the end of the 20 century, a fundamentally new method of diagnosis appeared based on nuclear magnetic resonance, which use was originally limited due to the low hardware and software support [3]. With the development of technical facilities and experience,the magnetic resonance imaging (MRI) is included in mandatory research protocols recommended by international urological associations [6].
Technique of magnetic resonance urography (MR urography) is based on obtaining high-intensity MR signal from the slow-moving or stationary liquid. A set of images taken in consecutive MRI scans is used for the construction of additional oblique views and three-dimensional image, and against the background of less intense tissue in the area of research we get sharper images of upper urinary tract. Not dilated urinary tract due to the small amount of liquid is visualized fragmentarily; sometimes it is not differentiated against of the surrounding structures. Accordingly, with the dilatation and increase of the liquid contents the MRI study allows establishing the degree of dilatation, its level and, in many cases, the cause of obstruction [4].
Best upper urinary tract visualization can be obtained at excretory MR urography using paramagnetic contrast agents and diuretic loading which makes possible to determine the functional state of the kidneys and ureters, visualize the bladder or urinary reservoir after intestinal plastic [3].
It should be emphasized that, unlike X-ray cystography, MRI allows evaluating the bladder in any projection and clearly identify pathological changes in the bladder wall, which is often the cause of ureterohydronephrosis [5].
Objective: To examine the anatomical and functional changes in the upper urinary tract using MR urography with the paramagnetic contrast agents and forced diuresis. Assess the effectiveness of MRI in the diagnosis of ureterohydronephrosis.
Materials and Methods
The results were analyzed of examination and treatment of 250 patients with invasive bladder cancer who were treated at the department of plastic and reconstructive oncourology since 2010 to 2012. In 75 cases the primary disease was complicated by ureterohydronephrosis. The age of patients ranged from 27 to 73 years. Men — 52 (69.3%), women — 23 (30.7%).
All patients were examined with the method of MR urography using hydrography mode on magnetic resonance imaging scanner of General Еleсtriс Signa Ovation 0.35T.
In all the cases, the adapted MRI protocols were used to assess the anatomic and functional status of upper urinary tract and bladder. Before being scanned, the patients underwent an anti-peristaltic diet as preparation to study.
The method is as follows: 30–40 minutes prior to scan the oral hydration of patients was performed. Patient is scanned lying on the back, arms along the body. Scanning is performed in the radio frequency coil forthe body. Synchronization with breathing is not used. The patient should lie still. Area of study necessarily involves the upper urinary tract and the bladder. The tomogram is done in three orthogonal projections.
To diagnose the condition of upper urinary tract the optimal scan marking was performed to obtain T2-weighted images in the coronal plane. Then the patients received Lasix at the rate of 0.8 mg/kg. Afterwards, the study protocol included scanning in the axial plane in T1 and T2-weighted images and in the sagittal plane in T2-weighted images. Further scanning was performed in the coronal plane in the mode of fat suppression with the study area including the upper urinary tract and the bladder. The protocol includes mandatory use of paramagnetic contrast agents (at the rate of 0.2 mg/kg) in T1-weighted images.
Position, shape, size, and condition of the upper urinary tract and the bladder were assessed before and after pharmacological test. In assessing ureterohydronephrosis, the thickness of the renal parenchyma was analyzed, as well as the extent and shape of the renal pelvis complex dilatation, the functional state of dilated ureter, and the level and cause of obstruction.
Results
As a result of the study the unilateral ureterohydronephrosis was diagnosed in 60 (80%) patients, and bilateral — in 15 (20%) patients.
Analysis of typical anatomical and functional changes in the upper urinary tract allowed dividing patients into 4 groups.
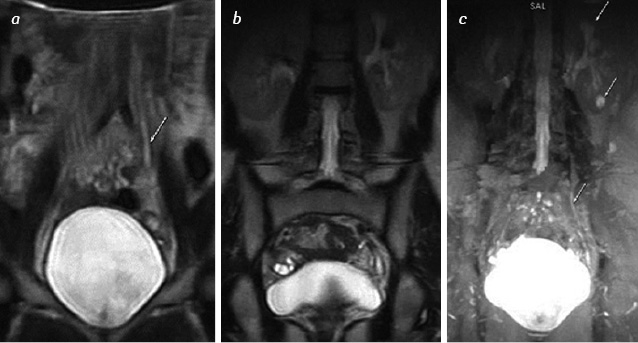
Characteristic feature of changes in the upper urinary tractin group1 of 24 (32%) patients wasa slight dilatation of the ureter, which is manifested in the form of stasis of urine. After intravenous Lasix administration the urine passes freely through the upper urinary tract. Renal parenchyma is preserved, the renal pelvis complex is not dilated (fig. 1).
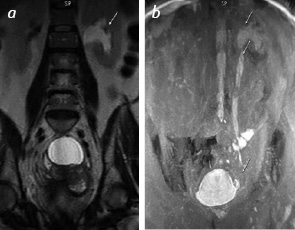
Group 2, of 27 (36%) patients,was characterized by dilatation through all the length of the ureter up to 15 mm of length. Renal parenchyma was preserved, with moderate dilatation of pelvis and calyces. After infusion of Lasix patients were divided into two categories: in 14 (52%) the increased diuresis and suprasthenic ureteral ectasia was observed, indicating a stable obstruction while maintaining the reserve function of kidney (fig. 2). In 13 (48%) the reduction of ectasia of upper urinary tract was noted due to compensated ureteral stricture in the distal third (fig. 3).
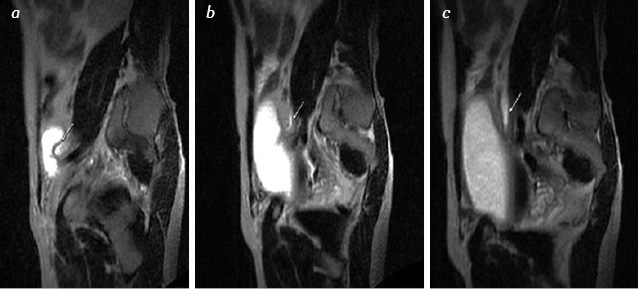
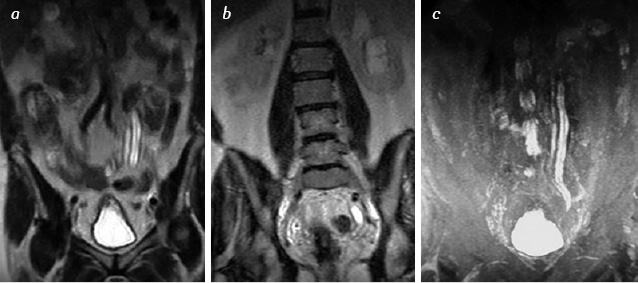
Group 3 (21 patients — 28%) was characterized by the growth of retention characteristics in the form of sustainable ectasiaof calyx-pelvis complex, the ureter dilated along the entire length, twisted. Infusion of Lasix showed itself not effective in 14 patients (65%), contractile properties of upper urinary tractwere absent. 7 patients (35%) manifested little effect, and chaotic contraction of the ureter. Due to changes the renal parenchyma is not uniformly thinned, visualized fragmentarily (fig. 4, 5).
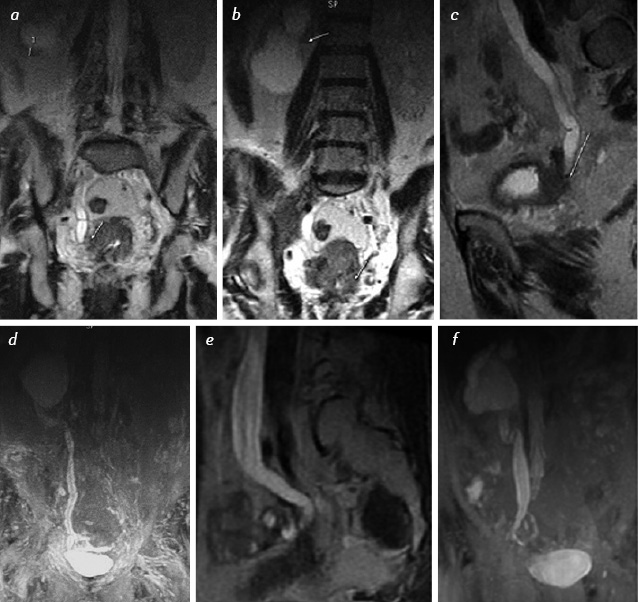
Group 4 (3 patients — 4%) was characterized by atony of dialtedafunctional ureter, renal parenchyma is thinned in the form of polycystic formation (fig. 6).
In all the cases when comparing the results of MRI before and after the administration of Lasix, a clearer visualization was noted of the upper urinary tract after Lasix infusion.
Thus MRI has exceptional opportunities for application, in case when it is not possible to perform the excretory urography, for example, for anafunctional kidney, at low urinary tract contrasting in renal failure.
Using MR urography with diuretic load we diagnosed the ureteral stricture in five cases.
In all the cases the MR imaging with MR urography allowed clearly establishing the level and in 92% of cases the cause of obstruction.
Conclusions
MR urography is a technique that allows you to visualize the upper urinary tract without invasive intervention, radiation exposure and contrast use. It is a highly informative method for studying the obstructive processes of the upper urinary tract that can be applied to patients with severe renal failure, with severe allergic reactions to iodine-containing contrast. Use of MR-urography allows, in addition to the level of obstruction and the degree of dilation of the urinary tract, to detect intra-and extra-abdominal causes of urine outflow. In addition to information about the urinary tract, MR-urography provides important information about the renal parenchyma, the processes occurring in the walls of the urinary tract and adnexa.
The use of MR-urography with diuretic load gives information about the anatomical and functional status of upper urinary tract.
References
1. Аляев Ю.Г., Синицын В.Е., Григорьев Н.А. (2005) Магнитно-резонансная томография в урологии. Практическая медицина, Москва, 270 с.
2. Терновой С.К., Аляев Ю.Г., Синицын В.Е. и др. (2001) Диагностические возможности и клиническое применение МР-урографии. Медицинская визуализация, 2: 72–77.
3. Труфанов Г.Е., Петров С.Б., Мищенко А.В. и др. (2008) Лучевая диагностика опухолей почек, мочеточников и моченого пузыря. «ЭЛБИ-СПб», Санкт-Петербург, 197 с.
4. Стаховський Е.О., Карпенко В.С., Пірогов В.О. та ін. (2000) Резервуарна функція сечового міхура. Урологія, 4: 21–25.
5. Cowan N.C., Turney B.W., Taylor N.J. et al. (2007) Multidetector computed tomography urography (MDCTU) for diagnosing upper urinary tract urothelial tumour. BJU Int., 99(6): 1363–70.
6. Lee K.S., Zeikus E., DeWolf W.C. et al. (2010) MR urography versus retrograde pyelography/ureteroscopy for the exclusion of upper urinary tractmalignancy. Clin. Radiol., 65(3):185–92.





Leave a comment